INSTRUCTIONS FOR SURGERY
The Night Before:
- A. Make sure to shower; wash hair and face.
- B. Eat and drink as usual. Take all medication unless otherwise instructed by your doctor.
The Day of Surgery:
- A. Nothing to eat or drink after midnight prior to procedure. Take all medications unless otherwise instructed. If you are an insulin-taking diabetic, take your insulin, test your blood sugar and write the results on a piece of paper to give to the nurse at the surgery center.
- B. Wear loose clothes and SHORT SLEEVES. Slacks are suggested for ladies. Tennis shoes or similar types of rubber-soled shoes are requested.
- C. Do not wear make-up, lotions, or cologne. Remove all jewelry and leave it at home. Medical alert tags and wedding rings are OK.
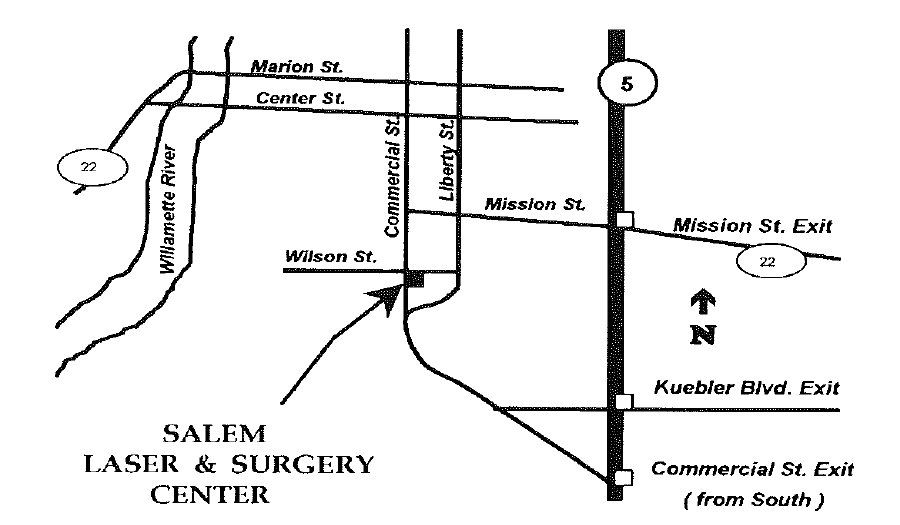
- D. In order to allow sufficient time for the admission procedures prior to your surgery, PLEASE ARRIVE AT THE SALEM LASER AND SURGERY CENTER at:
DAY
DATE
TIME
Becuase waiting room space is very limited, we ask that
only one person accompany you and that you arrive no earlier than the time indicated above. Thanks!
- You will not be allowed to drive yourself after you have surgery. Be sure you have someone to drive you home. If you plan to take a taxi home, you must have responsible adult (other than the driver) accompany you.
- Provide a responsible adult to transport him/her home from the facility and remain with him/her for twenty-four (24) hours, if required by his/her provider.
- Please bring: current medical insurance cards, and a photo ID (if this does not show your current address, you must also bring a utility bill or other correspondence which shows your current address).
Note: the photo ID is
necessary becuase we are now required to comply with federal indentity-theft prevention
laws. Also bring your glass case if you wear glasses.